In neurosurgery, the difference between a good outcome and a great outcome is often measured in millimeters. That's why, even when anatomical considerations seem straightforward, I use image-guided surgery on almost every case.
Why Use Navigation for "Routine" Procedures?
- Redundancy is safety. It provides a critical layer of verification that backs up my anatomical knowledge.
- Team synergy. Technology is only as good as the people using it. Frequent use builds muscle memory for the entire OR team, ensuring that when we face complex, high-pressure cases, the workflow is seamless.
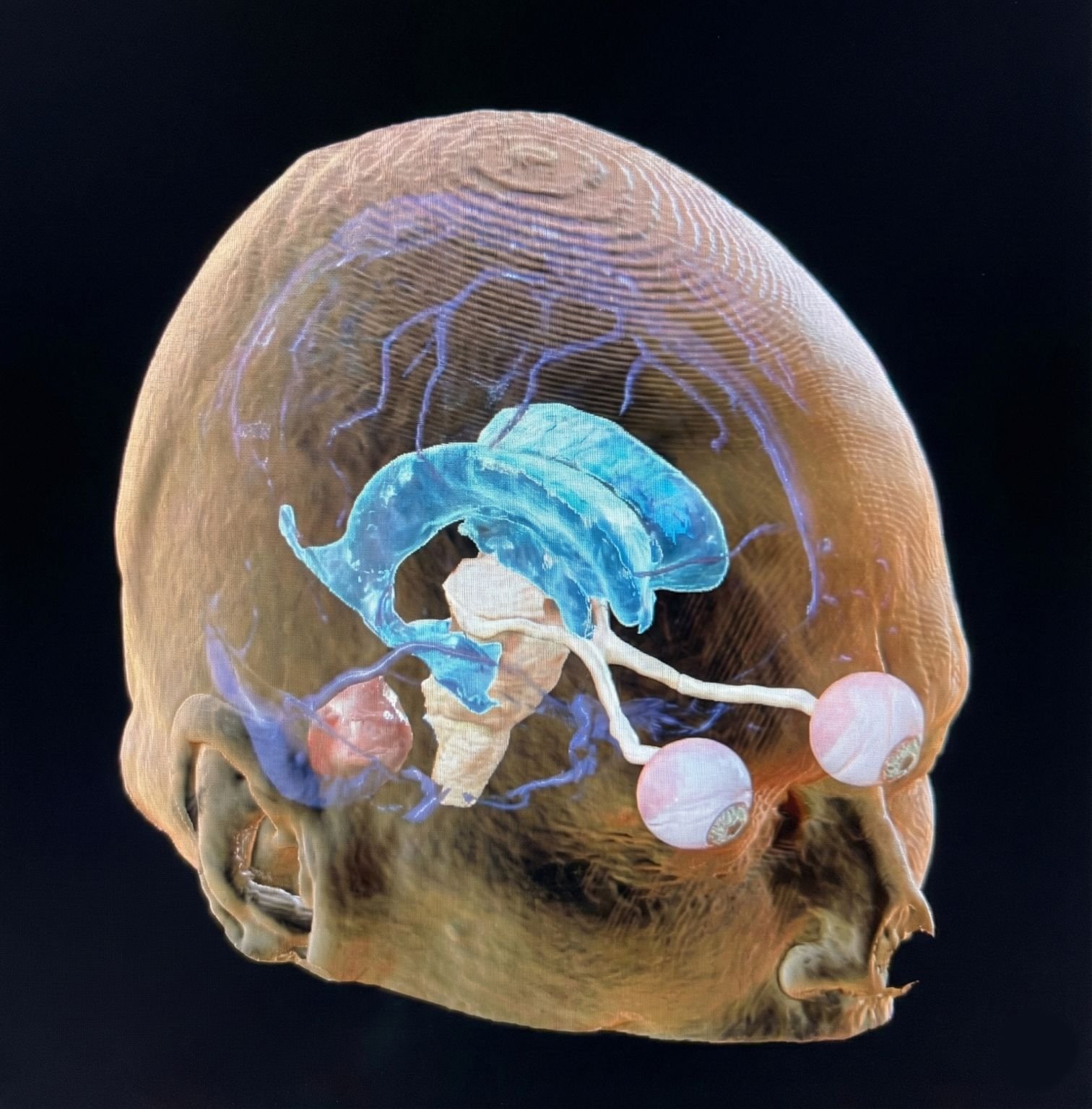
3D reconstruction showing the vascular anatomy and ventricular system — my roadmap for surgical planning.
Looking at this 3D reconstruction, you can see how I approach a case. I don't just look at the tumor; I look at the vascular anatomy to build my initial roadmap. Whether I'm planning a craniotomy, an endovascular approach, or a radiosurgery plan, the questions are always the same: What is the target, and what is the safest corridor to reach it?
The Limitation of Standard Navigation
The limit of standard navigation, of course, is that it relies on static images. The moment the dura is opened and fluids drain, the brain shifts. This is where live intraoperative imaging bridges the gap.
I view the ability to fuse live ultrasound with pre-op data as the next big advancement in surgery, giving us a real-time, updated map.
It is still the art of medicine, just enhanced by the precision of technology.